Tennis elbow, or lateral epicondylitis, is a very painful musculoskeletal condition of the elbow, classified as a tendinopathy. It is commonly caused by repetitive activity of the forearm, resulting in overuse of the "extensor" muscles and forming small tears, especially in a place where tendons are attached to the lateral epicondyle.
Common symptoms of tennis elbow:
- pain and burning sensation along the outside of the forearm and the elbow;
- weaker grip strength;
- symptoms are often worsened with increased forearm activity.
-
To date, the best therapy solution for this condition has not been proposed nor validated. Most of the current treatment modalities are either insufficient or bring only short-term improvement. Recently, more and more studies have emphasized the effectiveness of Radial Shock Wave Therapy (RSWT®) in managing chronic tendinopathies.
The main goal of this study was to compare the efficacy of physical therapy combined with RSWT® with physical therapy alone on tennis elbow.
Methods
A total of 30 participants with lateral epicondylitis were enrolled in the study and divided into two groups:
- control - received physical therapy* (3 sessions per week over 3 weeks) plus “placebo”** shockwaves;
- experimental - received physical therapy (3 sessions per week over 3 weeks) and RSWT® - 3 weekly sessions (once a week); 2000 impulses at 10 Hz frequency with maximally tolerated pressure (average 3.1 bar).
*Physical therapy consisted of ultrasound diathermy, transcutaneous electrical nerve stimulation, static stretching exercise plus transverse friction massage on the involved elbow over the common extensor tendon. Same program was administered in both groups.
**Shockwaves without any pneumatic pressure.
Radial extracorporeal shock waves were applied using the DolorClast® Radial Shock Waves device (Electro Medical Systems, Nyon, Switzerland).
Outcomes
All participants received detailed baseline (T0) evaluation and were reassessed in certain follow-up periods: 6, 12, and 24 weeks after treatment.
Starting from baseline, each study checkpoint protocol included:
- pain intensity measurement via Visual Analog Scale (VAS);
- assessment of the maximal grip strength;
- determination of the upper extremity disability and symptoms using the Taiwan version Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire;
- ultrasonography - 2D image of common extensor tendon and real-time sonoelastography.
Results
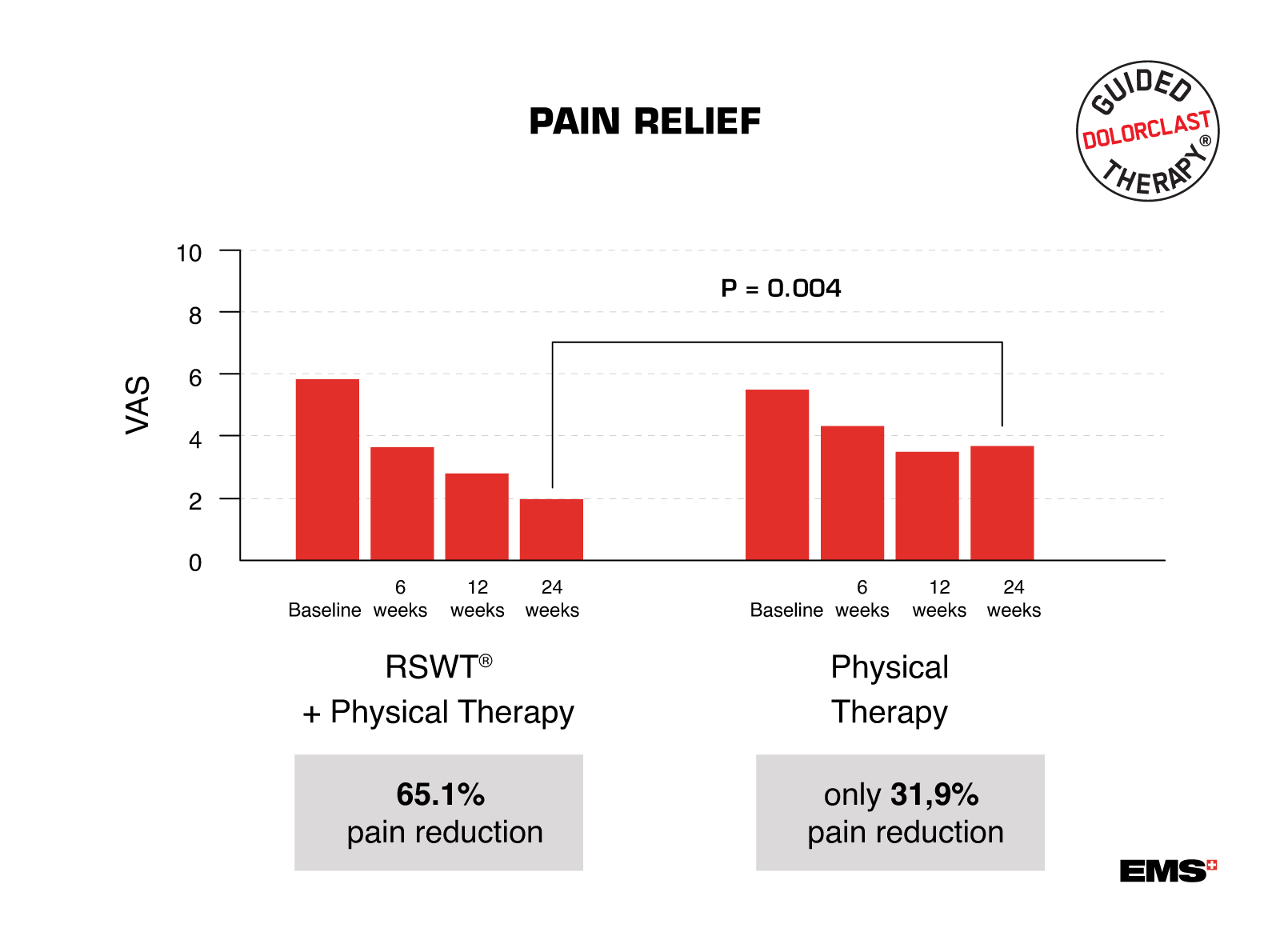
65% vs. 32% pain reduction after 24 weeks of treatment with combination therapy!
RSWT® combined with physical therapy resulted in significant pain reduction at each study checkpoint. Pain level on VAS decreased faster and more progressively in the experimental group than in controls. At the end of the follow-up (24 weeks after the treatment), the mean VAS score was significantly lower in the group that received combined therapy.
Outcomes
All participants received detailed baseline (T0) evaluation and were reassessed in certain follow-up periods: 6, 12, and 24 weeks after treatment.
Starting from baseline, each study checkpoint protocol included:
- pain intensity measurement via Visual Analog Scale (VAS);
- assessment of the maximal grip strength;
- determination of the upper extremity disability and symptoms using the Taiwan version Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire;
- ultrasonography - 2D image of common extensor tendon and real-time sonoelastography.
Results
65% vs. 32% pain reduction after 24 weeks of treatment with combination therapy!
RSWT® combined with physical therapy resulted in significant pain reduction at each study checkpoint. Pain level on VAS decreased faster and more progressively in the experimental group than in controls. At the end of the follow-up (24 weeks after the treatment), the mean VAS score was significantly lower in the group that received combined therapy.
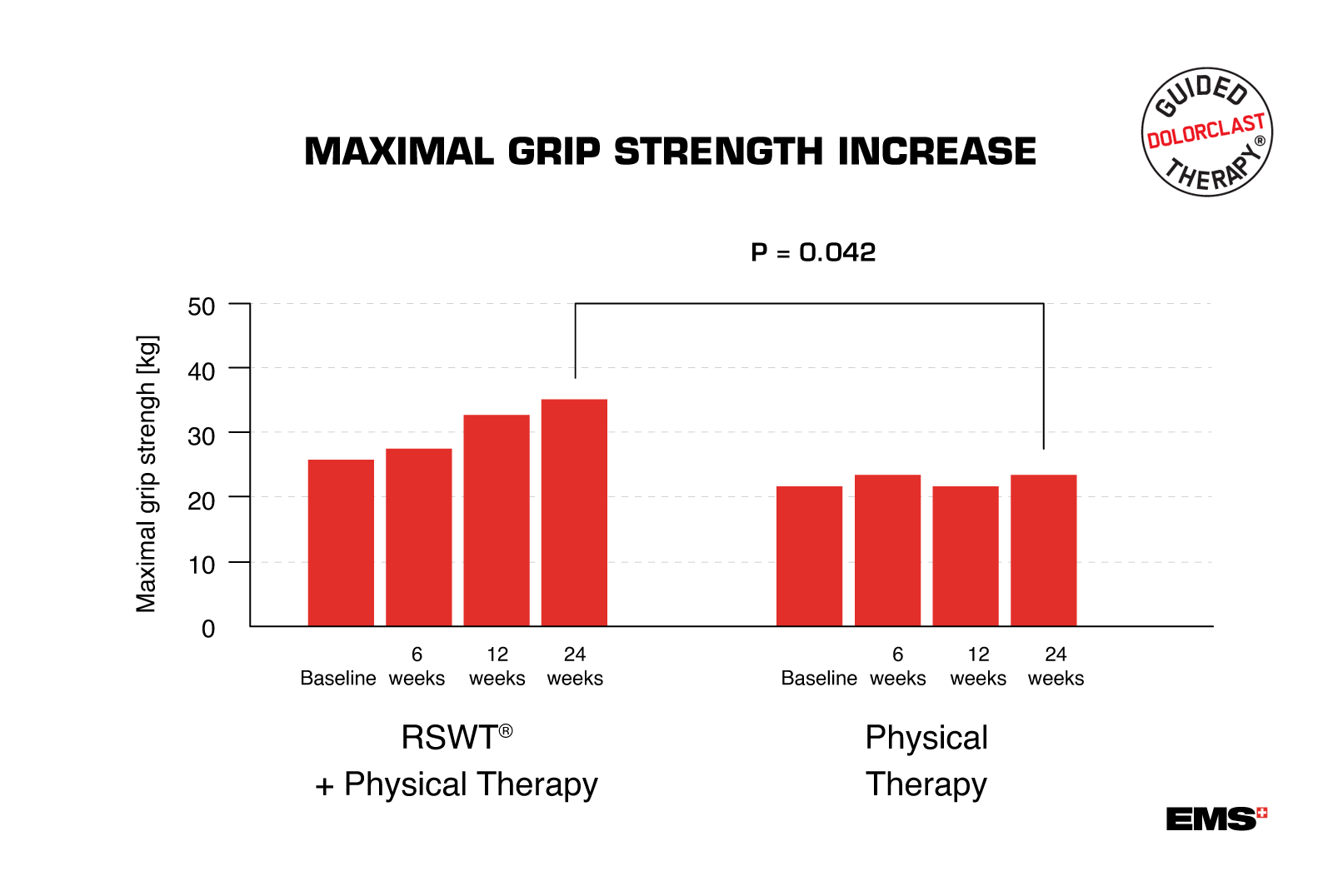
Maximal grip strength has also significantly increased during the study. Its improvement was statistically more pronounced in weeks 12 and 24 after the treatment with RSWT® than in the control group at the corresponding time.
DASH disability/symptom scores were significantly lower in the experimental group at each study checkpoint compared to the control group.
Only in group with the combination therapy, the tear size of the tendon (assessed with ultrasound) gradually decreased over time, and appeared to be fully healed at the end of the follow-up!
Conclusion
Combining RSWT® with traditional physical therapy is superior to conventional physical monotherapy and significantly reduces pain intensity caused by tennis elbow, increases maximal grip strength, and improves upper extremity function and work performance. Treating lateral epicondylitis with RSWT® helps overcome inconvenient symptoms and brings remarkable benefits for patients in tendon healing!
Discover the full potential of Guided DolorClast® Therapy - learn how to address 90% of all major musculoskeletal disorders with success using combination therapy!